

"In primary care I often see early signs of metabolic decline — persistent fatigue, reduced cellular energy, gradual shifts in systemic balance. In critical care transport, I encounter individuals further along the same spectrum. The difference in presentation is striking."
My clinical work has given me perspective across different stages of metabolic health. In primary care settings I observe gradual shifts in metabolic balance. On mobile ICU transport I encounter more advanced presentations along the same continuum. Both inform how I think about botanical metabolic support strategies alongside current daily routines.
Why Delivery Route Can Matter for Certain Compounds
Many nutritional compounds must survive a challenging journey through the digestive tract before they can be absorbed into the bloodstream. The environment in the stomach — highly acidic, with gastric acid maintaining a pH range of approximately 1.5 to 3.5 — and the subsequent passage through the liver can significantly reduce the amount of active compound that ultimately reaches systemic circulation [1].
Research in clinical pharmacokinetics has long examined how different administration routes affect how much of a compound becomes available in the body. For some substances, this "first-pass" effect through the digestive system and liver can be substantial. Understanding these mechanisms may help inform more thoughtful decisions about supplement delivery forms.
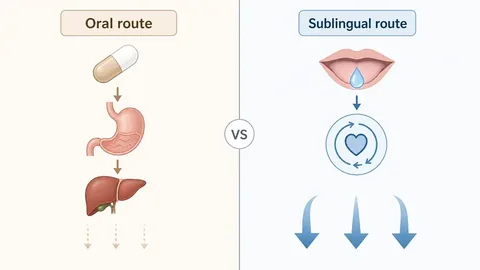
Common Challenges with Standard Oral Delivery
Standard capsules and tablets are exposed to gastric acid in the stomach (pH 1.5–3.5) and then undergo hepatic first-pass metabolism before reaching systemic circulation [2]. Pharmacokinetic research indicates that this combination can result in a meaningful reduction of the active ingredients before they reach general circulation.
The liver's enzymatic processing — particularly through cytochrome P450 systems — may metabolize a significant fraction of absorbed compounds before those compounds reach their target tissues [1]. The degree of hepatic first-pass metabolism varies by compound structure, individual enzyme activity, dose, and concurrent medications, but the pharmacokinetic principle is well established in clinical literature.
Individual responses vary widely depending on formulation quality, the specific compounds involved, and personal physiological factors. There is no universal guarantee of absorption efficiency — but understanding the barriers may help explain why some individuals report limited perceived benefit from standard oral supplements.
Labeled Ingredient Disclosure
| Ingredient (as labeled) | Botanical / Chemical Name | Form |
|---|---|---|
| Eleuthero | Eleutherococcus senticosus | Root extract |
| Coleus | Coleus forskohlii | Root extract |
| Maca Root | Lepidium meyenii | Root extract |
| African Mango | Irvingia gabonensis | Fruit extract |
| Guarana | Paullinia cupana | Seed extract |
| Ginseng | Panax ginseng | Root extract |
| Gymnema Sylvestre | Gymnema sylvestre | Leaf extract |
| Chromium | Chromium picolinate | Trace mineral |
As labeled on the manufacturer's product. Serving sizes and full amounts are on the official product page. Not independently verified by this publication.
Learn more about the botanical sublingual formula referenced in this report.
See the Recommended Sublingual Formula → Opens manufacturer's page · Affiliate link · 60-Day GuaranteeThe Pharmacokinetic Rationale for Sublingual Administration
Sublingual delivery places a liquid or dissolvable formulation beneath the tongue, where it can be absorbed through the sublingual mucosal membrane — a tissue that is notably thin (approximately 100–200 micrometers) and highly vascularized [3]. From there, compounds may enter the sublingual venous plexus and travel through the venous drainage of the oral cavity into the internal jugular vein — bypassing much of the gastric degradation and initial hepatic first-pass metabolism for a portion of the dose [3].
Physiological data suggests that sublingual delivery may allow faster absorption via this route and more direct systemic entry for certain compounds compared with standard oral capsules [3]. The degree of absorption depends on several formulation-specific and physiological factors, including lipophilicity, molecular size, dissolution rate, and contact time under the tongue.
Pharmacokinetic studies have explored the sublingual and buccal mucosal routes for various substances because they may offer more direct entry into systemic circulation for suitable compounds [2][3]. Results remain formulation-dependent, and individual physiological factors play a significant role. This does not guarantee any specific outcome, but it provides a rational, evidence-based foundation for considering sublingual formulations as part of a metabolic support strategy.
For compounds known to have poor oral bioavailability — due to either gastric acid degradation or extensive hepatic first-pass metabolism — the sublingual route offers a pharmacokinetically sound delivery alternative that merits consideration [3].
Access the botanical sublingual formula that accompanies this clinical review, prepared with the delivery principles described above. Backed by a 60-day unconditional money-back guarantee.
Access the Botanical Sublingual Formula → ⭐ 4.8/5 · 194k+ customers · Made in USA · Secure Checkout · Affiliate link